Crouse Protocol for Reversing MCI and Preventing Alzheimer’s
Chapter 11 From the book: Increasing IQ, Cognition and COVID-19 Cure Rate with Essential Nutrients……..Targeted Detox Improves Children’s IQ, ADHD Behavior, and Adult Cognition
by Dennis N Crouse
My interest in MCI and AD began in the fall of 2012 when my mother turned 86. We noticed she could only talk about what happened in the distant past not what happened in the recent past, such as earlier in the day. She had quicky lost her short-term memory and could no longer perform some daily living skills, such as sewing and balancing the checkbook. For her that was very frustrating because she had worked as both a seamstress and book keeper. For me this was disturbing as I knew how badly this might end if her condition progressed into dementia. My mother was diagnosed with MCI that was a likely precursor of AD and was prescribed Aricept (a.k.a. Donepezil). In order to help my mother, I decided to begin a multi-year journey into understanding the cause of her cognitive impairment. The first stop on my journey was to check the efficacy of the cholinesterase inhibitor Aricept that was prescribed for my mother.
Efficacy of Cholinesterase Inhibitors and Memantine
Many people with mild cognitive impairment (MCI) and mild Alzheimer’s disease (AD) are prescribed a cholinesterase inhibitor (ChEI). Those with moderate to severe AD (e.g., Mini-Mental State Examination [MMSE] scores below 15) are prescribed memantine, with in some cases a ChEI. Administration of a ChEI increases the concentration of acetylcholine by inhibiting its breakdown. These drugs treat some of the symptoms of MCI, such as memory loss, agitation, apathy, and psychotic symptoms including delusions, hallucinations, and disordered thought. Examples of ChEIs are:·
Galantamine (trade name Razadyne) is approved by the FDA for treatment of vascular dementia and mild to moderate AD. It enhances memory in brain-damaged adults544.·
Rivastigmine (trade name Excelon) is approved to for mild and moderate AD.·
Donepezil (trade name Aricept) is approved to treat all stages of AD.A study was published in 2011 on the efficacy of these three ChEIs and memantine taken by patients diagnosed with MCI or mild AD.
A study was published in 2011 on the efficacy of these three ChEIs and memantine taken by patients diagnosed with MCI or mild AD. Approximately one-half of 392 MCI patients and two-thirds of 188 mild AD patients were APOE-4 carriers. Among the MCI patients 33.4% received only ChEIs, 11.7% received ChEIs and memantine, and 54.9% received neither. Among the 188 AD patients 38.9% received ChEIs, 45.7% ChEIs and memantine, and 15.4% neither817.
The patients with MCI were divided into three groups, only 22% of the non-treated group progressed to dementia, 43% of the ChEI treated group progressed to dementia, and 56% of the group treated with both memantine and ChEI progressed to dementia. Therefore, there is a greater risk of dementia among people taking these drugs. The mean time to dementia was 30% quicker in the ChEI treated group than the untreated group and 42% quicker for the memantine and ChEI treated group than the untreated group. Both MCI patients and AD patients who received ChEI treatment had a more severe decline in cognition than untreated patients. Therefore, these drugs may reduce symptomology of MCI and AD but both increase the risk of dementia and hasten the progression to dementia when compared with un-treated people817.
I have an acquaintance with MCI who was prescribed Aricept to improve her short-term memory but had trouble sleeping once she began taking the drug. The doctor then recommended a sleeping pill with the side effect of memory impairment. This is an example of a doctor being uniformed on the negative side effects of a prescribed drug.
Although these drugs are FDA-approved for those with MCI and AD, they are not efficacious for slowing the progression to dementia. In fact, they significantly increase the risk and speed the progression to dementia. These drugs will facilitate the progression to dementia quicker than no treatment. I recommended my mother not take Aricept!
Finding the Cause of MCI and AD
I realized that doctors had no efficacious solutions to my mother’s steep slide into MCI and AD. The only chance my mother had was to find the cause of her MCI. The results of this search for a causal factor are described in detail in chapter 2 of this book and in my book “Prevent Alzheimer’s Autism and Stroke”. Even though more than 30 genes have been correlated with AD, their role is limited and the major cause of AD is not currently believed to be genetic. The presenilin genes have been correlated with familial AD but only account for 0.5% of the cases. The APOE-4 gene increases the risk of AD by 50% but occurs in less than 20% of the population24. But in 2002 approximately 30% of the people over 80 had AD24. Therefore, the primary cause of sporadic AD is very likely an environmental factor rather than a genetic factor24. This conclusion is supported by the exponential increase in AD cases in the U.S. (see figure 7) as genetic mutations of human DNA causing disease do not spread exponentially.
This book is a summary of environmental factors known to negatively impact cognition. Aluminum is the xenobiotic with the most epidemiological, laboratory, and clinical evidence implicating it as the primary causal factor of AD (see chapter 2 -Cognitive Decline in Alzheimer’s Disease). Like the APOE-4 gene, aluminum also causes increased beta-amyloid in the brain79,80. Aluminum also binds to oligomers of beta-amyloid to make droplets that are more neurotoxic than beta-amyloid81,721. Aluminum accumulates in the brain with age due to increased gastrointestinal absorption of aluminum over age 70 and weakening of the blood-brain barrier in those, like my mother, with vascular disease84,85,818. A meta-analysis of studies involving 1,208 participants including 613 AD patients revealed aluminum is higher than normal in brains, serum, and cerebrospinal fluid of AD patients compared with non-AD patients819.
Crouse Protocol
In order to reverse my mother’s MCI, my protocol was designed to decrease brain drainers, such as aluminum, that had accumulated in her brain and improve her vascular system by lowering both aluminum and serum homocysteine.
The amount of aluminum in her diet and brain had to be reduced in order for her hippocampus to make more neurons than it was losing to this xenobiotic neurotoxin. This could potentially increase both her hippocampal volume and short-term memory. With more new neurons the hippocampus can make neural networks for short-term memory storage and add plasticity to the brain to repair the atrophy caused by brain drainers. With the simple strategy of decreasing the ingestion and targeting the detox of brain drainers, such as aluminum, and daily augmenting with proven nootropics, some of which lower homocysteine and improve her vascularity, my mother recovered her short-term memory.
This targeted aluminum detox must be helped by eliminating aluminum from the diet (see chapter 9 and appendix IV for sources of aluminum). The main sources of aluminum discovered in my mother’s house were:·
Aluminum cooking pots and heater in coffee maker·
Aluminum containing baking powder·
Aluminum antacids·
Aluminum in tap water
Augmenting with 5 Brain Savers
With the help of numerous researchers having published clinical studies on humans, I had the data I needed to develop a protocol for my mother that reversed her declining MCI. The protocol includes augmenting her diet with brain savers to eliminate brain drainers and nootropics to enhance the vascular system, hippocampal neurogenesis, and mitochondrial biogenesis.
Orthosilicic acid (OSA) is the most important part of the protocol. It is recommended to daily drink 3 to 4 cups of greater than 49ppm OSA rich water for targeted aluminum detox (see appendices I, II, and III for sources of OSA). My mother has been supplied with Fiji water delivered to her door as her source of OSA and encouraged not to drink tap water. Fiji water contains less than 0.2ppm of fluoride820 while in 2012 mother’s tap water contained 1.0ppm.
L-selenomethionine augmentation is also important part of the protocol. My mother has amalgam fillings and is being constantly exposed to mercury. In addition, the elderly can boost their immunological system by augmenting with selenium for improved immunity to viral infection. It is recommended to augment daily with 100 to 200mcg of L-selenomethionine.
Vitamin B1 (a.k.a. thiamine) augmentation is important for enhancing lead elimination (see Targeted Detox of Lead in chapter 4). It is recommended to augment with vitamin B1 50 – 100mg for adults twice a day (morning and evening) or a prolonged or time-released B50 or B100 complex once a day.
Vitamin B3 (i.e., niacin or nicotinamide) augmentation is important for enhancing PCB elimination (see Targeted Detox of PCBs in chapter 4). It is recommended to augment with vitamin B3 as niacin or niacinamide 50 – 100mg/day prolonged or timed release as part of a B50 or B100 complex once a day.
Zinc augmentation is important for enhancing lead elimination with vitamin B1 see Target Detox of Lead in chapter 4). It is recommended to augment with 25 – 30mg/day as a chelate (see Section on Zinc Augmentation in Chapter 7). Note that zinc is also a nootropic as it is required for enzymes that metabolize homocysteine to methionine for vascular health. Zinc augmentation can also protect the blood-brain barrier from aluminum toxicity818.
Augmenting with 9 Nootropics
As pointed out in chapter 2 both vascular (i.e., white matter intensities) and AD (i.e., accelerated hippocampal atrophy) pathologies are most commonly linked to MCI. A healthy vascular system and hippocampus are both required for short-term memory. White matter lesions in the vascular system of the brain caused by high plasma homocysteine levels may be a causal factor of my mother’s rapid loss of short-term memory at age 86. The following nootropic vitamins and essential nutrients for vascular health protect my mother from further cognitive decline and possibly enhance her cognition (see chapter 10 on nootropics):·
Vitamin B6 (a.k.a. P-5-P Pyridoxal-5-Phosphate) – 50 – 100mg/day prolonged or time released (B50 or B100 complex)·
Vitamin B12 – 500mcg – 1mg/day as methylcobalamin capsules, tablets, or sublingual lozenges (in addition to 50 – 100mcg of cyanocobalamin in a B50 or B100 complex)·
5-MTHF(a.k.a. Methyl Folate) – 400mcg/day, if taking a B50 of B100 complex with 400mcg of folic acid, otherwise take 400mcg to 1mg/day of 5-MTHF·
TMG(a.k.a. Trimethylglycine) – 500mg/day (not recommended for diabetics)
The protocol included additional nootropics that enhance cognition by increasing neurogenesis and mitochondrial biogenesis. They include the following (see chapter 10 on nootropics):·
PQQ for NGF production, neurite growth, and mitochondrial biogenesis – 20 – 25mg/day·
CoQ10 for increased mitochondrial energy production – 400mg of CoQ10 per day as ubiquinone or 200mg of CoQ10 as ubiquinol the reduced form of CoQ10·
Vitamin K2-MK-4 for increased neurogenesis and xenoprotection – 5mg – 15mg of vitamin K2-MK-4 and 60mcg – 90mcg of vitamin K2-MK-7 (not recommended for those on anticoagulants)·
Taurine and aerobic exercise for BDNF production and increased neurogenesis – 1.5gr./day of taurine as powder or capsules and 40 to 50 minutes of aerobic exercise three times a week·
Lutein for stimulated BDNF production and increased neurogenesis – 10-40mg/day of lutein and 1-5mg/day of zeaxanthin
Augmenting with Vitamins D3 and K2-MK-4 for Increased Bone Mineral Density
My mother, like many postmenopausal women, has osteoporosis in her lumbar spine that is characterized by porous bones of low bone mineral density (BMD below 0.83 gr/cm2). Porous bones are more prone to fractures and these fractures are a leading cause of disability and mortality in the elderly821. Incredibly, a recent study found 25% of people between 35 to 40 years of age have weaker than normal bones822. This is called osteopenia (BMD below 0.98 gr/cm2) and if untreated can lead to osteoporosis. There is currently a treatment for both osteopenia and osteoporosis that results in increased BMD and bone strength823-825. The treatment involves augmentation with both vitamin D3 and the nootropic vitamin K2-MK-4.
Two independent clinical studies on groups of women 50 to 80-years old with osteopenia or osteoporosis showed that simultaneous daily augmentation with both vitamin D3 (1.0mcg/day 40 IU) and vitamin K2-MK-4 (45mg/day) for at least 6 to 12 months significantly increases vertebral (lumbar spine) BMD by 4 to 6%, respectively. Continued augmentation beyond the first year resulted in vertebral BMD stabilizing at the higher level. Taking only vitamin D3 or only vitamin K2-MK-4 showed no significant improvement in BMD, however, augmentation with vitamin K2-MK-4 alone did stabilize vertebral BMD over a two-year period823-824.
Surprisingly, augmentation with just calcium lactate (2gr/day) showed a significant decrease in vertebral BMD over a 2-year period824,825. Augmentation with vitamin K2-MK-4 not only prevents loss of vertebral BMD823-825 but also reduces vertebral fracture incidence825. With calcium augmentation (150mg/day) there were 30 vertebral fractures in a 2-year period while with K2-MK-4 augmentation (45mg/day) there were only 13 vertebral fractures in the same period825. There would likely have been even a lower incidence of vertebral fractures had both vitamin D3 (50mcg/day) and vitamin K2-MK-4 (15mg/day) been augmented simultaneously.
There is a synergy between vitamins D and K that promotes calcium deposition in the bones and prevents and even reverses calcium deposition in the cardiovascular system826. It has been shown that 3-years of vitamin K2-MK-7 (180mcg/day) reverses arterial stiffness (i.e., hardening of the arteries) in postmenopausal women827. Since vascular cognitive impairment (VCI) is a causal factor of MCI (see Chapter 2), both a daily vitamin D3 (50mcg/day 2,000 IU) and vitamin K2-MK-7 (180mcg/day) are recommended for improved cardiovascular health.
Helping My Mother Implement the Crouse Protocol
Eight years have gone by since we noticed my mother’s lack of short-term memory. My mother is now 94 and still living in the same house she has lived in for the last 40 years. Her short-term memory improved while on the protocol, her MMSE (Mini-Mental State Examination) score slightly increased, and she has successfully used the sewing machine on a few occasions. She lived through a week without electricity after the most damaging wind storm (i.e., derecho) in the last 100 years blew through her town. She remains fiercely independent in spite of being handicapped by residual memory deficiencies. She has kept her resiliently and is willing to remain on the protocol and take care of herself and her three cats. I pack her brain savers, nootropics, and vitamin D in plastic bags and call daily checking to see if she has remembered to take them and drink the Fiji water. Thankfully, usually she has remembered.
Anecdotal Information Regarding the Crouse Protocol
The following anecdotal information is from a Facebook group moderated by my wife titled “Alzheimer’s: Late and Early Onset, APOE-4” focused on preventing Alzheimer’s in those with APOE-4 and treating patients diagnosed with early and late onset Alzheimer’s disease:
“I have been meaning to follow-up with you regarding my Mother. I arrived in Kansas on September 13th and within 48 hours I had my Mom on Fiji water, PQQ 20mg, and Q10 200mg. Included in her supplements I added a B-complex to be sure she got all the B vitamin’s… At almost exactly 2 months it was apparent that changes were taking place. My father even noticed and mentioned the changes… The changes include: She is much more communicative, involved in conversation, remembering events and telling stories, laughing, and joking. She is no longer incontinent and knows when she has to go to the bathroom. Rarely does she have an accident whereas prior we could be changing her 7 to 10 times a day… She no longer just stares off like she isn’t there… Her short-term memory is poor but her whole personality has mostly returned … I do believe the Fiji water and supplements you recommended have made a big difference… I wish to give hope to others that while I don’t believe Mom is “cured” she certainly has a much better quality of life than before I arrived to help and it has certainly made it ALOT easier for the caregiver.” Jan 2021
Conclusion Helping Others Implement the Crouse Protocol
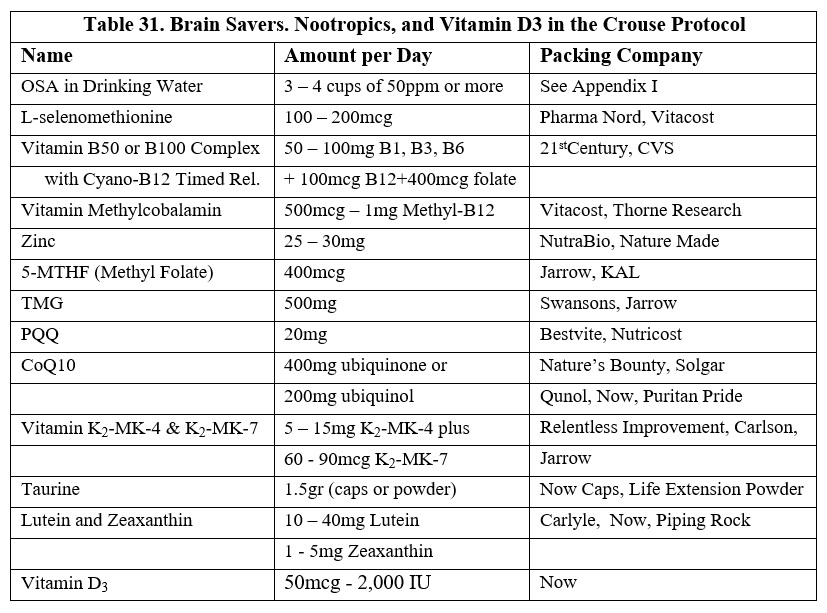
I have written this book to inform others about this protocol. I can only hope that this protocol will help others stop and possibly reverse the slide into AD as it has for my mother. The following table is a list of brain savers, nootropics, vitamin D3, and companies that currently pack them:
Here is a way to reduce the number of pills for the Crouse Protocol. You can take 3 pills and get all the supplements in the protocol except Vitamin K, TMG and Taurine. One is a multivitamin and the other contains PQQ and CoQ10 (take 2). see photos below
There are additional vitamins and minerals in the multivitamin that are not part of the protocol.